




The Right Ventricular outflow tract : the most desirable site for true septal spacing – A single operator experience

A Retrospective observational follow-up study was conducted on 140 cohort cases, who underwent RVOT (Right Ventricular Outflow Tract) Septal pacing, for class I indication for pacemaker implantation performed by a single operator. The purpose of the study was to demonstrate the ease of positioning a lead in the RVOT septum and to determine immediate and long term effects of Right Ventricular Outflow Tract Septal pacing in terms of pacing parameters and lead stability. The paper on ‘The Right Ventricular outflow tract : the most desirable site for true septal spacing” by Dr. V. Rajashekhar , Senior consultant Interventional Cardiologist & Electrophysiologist, was presented an ‘Outstanding Paper Award’ by Asia Specific Heart Rhythm Society Scientific Session for it’s high degree of effort toward technical, educational, or managerial achievement through its publication.
INTRODUCTION:
Right Ventricular Outflow Tract(RVOT) Septum has been proposed as a preferred site for right ventricular lead placement. However, techniques and methodology of positioning the lead in RVOT septum have not been well validated. Data concerning lead performances and complications for lead repositioning with this technique were deficient.
METHODS:
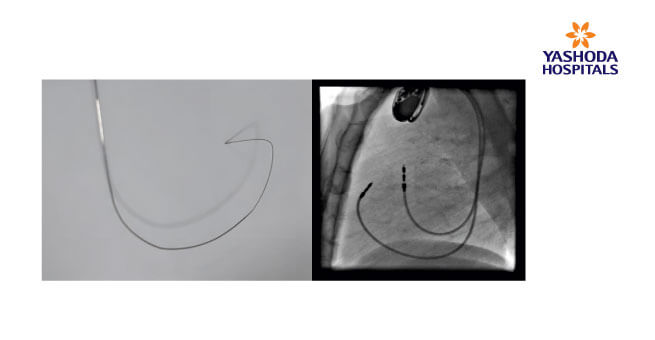
This was a Retrospective observational follow-up study that included a cohort of 140 cases, who underwent RVOT (Right Ventricular Outflow Tract) Septal pacing, for class I indication for pacemaker implantation performed by a single operator. Lead positioning was achieved by the means of a custom shaped style (lmage 1) as described by Harry Mand et al and optimal position was confirmed with the use of fluoroscopy in the anteroposterior and lateral projections(lmage 2). 1-year follow-up information on stimulation threshold, R-wave sensing, lead impedance, and lead complications were collected. Information was obtained on ventricular lead performance at implant, at 6-month and at 12-month follow-up, Statistical analysis was done using Microsoft Windows 7 software Statistical test applied were ANNOVA test ,Ttest, Jarque-Bera test.
RESULTS:
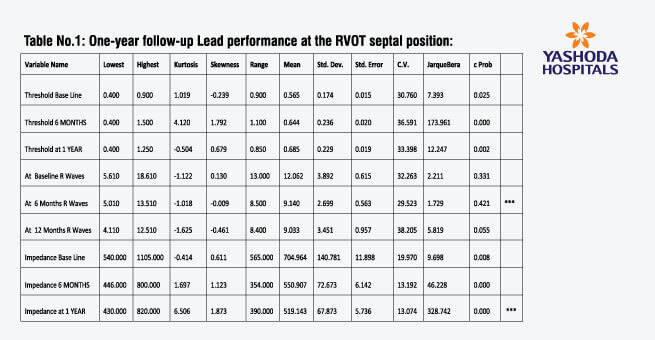
Lead performance at the RVOT septal position was stable at 1-year follow-up. Ventricular electrical parameters were acceptable with stable 1-year stimulation thresholds, sensing, and impedance for all lead types. One-year results demonstrated a mean stimulation threshold of 0.68V (+0.23V), mean R wave of 9.03 mV (+3.45 mV), and mean impedance values of 519.140 (+67.870). There were no cases of high pacing thresholds or inadequate sensing. There were no known patient deaths related to pacemaker complications.
CONCLUSION:
This study confirms that RVOT septal pacing can be achieved fairly rapidly and efficiently by use of stylet that can be shaped in the cath lab and optimal position achieved with satisfactory long term performance. The RVOT septum has emerged as an attractive site,which is technically easy to reach as the right ventricular ape. Successful implantation within the RVOT is readily achievable, but requires an understanding of RVOT anatomy and specific stylet shaping. The selection of the RVOT septum as the primary pacing site in the majority of patients with bradycardia indications was supported that indicates that long term electrical performance at this site is favorable.
About Author –
Dr. V. Rajasekhar, Consultant Interventional Cardiologist, Yashoda Hospital, Hyderabad
MD, DM (Cardiology)











{kind=link}